

Procedure
Ultrasound for Endometriosis Diagnosis and Surgical Planning
Advanced pelvic ultrasound helps detect signs of deep endometriosis, guiding accurate diagnosis and supporting surgical planning by Dr Michael Wynn-Williams.
“Diagnosis is Treatment”
Diagnosis of Endometriosis with Transvaginal Ultrasound (TVUS) has, for a long time, been considered the gold standard of diagnosing endometriosis. Since the early 2000s, there has been a significant improvement in the diagnosis, staging, and ability to plan surgical intervention – through using the technique of transvaginal ultrasound (TVUS). It is important to note straight away that a negative finding with TVUS does not necessarily mean that you don’t have endometriosis; an ultrasound performed through the abdominal wall is not accurate enough to rule out pelvic endometriosis.
Dr Wynn-Williams has extensive experience in performing a TVUS on superficial, deep infiltrating endometriosis (DIE), and ovarian endometrioma. Resent research has shown that having the capacity to perform the diagnostic endometriosis ultrasound during the patient examination process significantly enhanced the patients’ experience. Endometriosis TVUS enables Dr Wynn-Williams to plan the extent of often very complex pelvic surgery.
More Information about Ultrasound for Endometriosis Diagnosis
-
Superficial endometriosis, which affects approximately 80% of women with endometriosis, presents as shallow lesions along the peritoneum that have traditionally been challenging to detect with imaging. Through specialized expertise and advanced ultrasound techniques, Dr. Wynn-Williams can identify specific ultrasound features of superficial endometriosis, including hyperechoic foci, small cystic lesions, and peritoneal changes in areas such as the pouch of Douglas. While TVUS shows promise for non-invasive diagnosis of superficial endometriosis, it’s important to understand that a negative ultrasound does not rule out the presence of endometriosis.
-
Endometriosis tissue will typically grow in areas deep in the pelvis, such as behind the uterus, between the vagina and rectum (Pouch of Douglas), in the rectum, the ovaries, and the bladder. Deep infiltrating endometriosis is the definition given to endometriosis that has invaded at least 5mm deep into the tissue. Often, it is only the most experienced practitioners who can spot these areas of deep endometriosis when they position the ultrasound probe up against the diseased regions, through the back of the vagina. The areas of endometriosis appear as darker patches as they are denser with the scar tissue they contain. Because Dr Wynn-Williams performs surgery and excises endometriosis without delay - often only a few days after he has completed the ultrasound scan - he is continuously improving his skill in recognising lesions of deep infiltrating endometriosis.
-
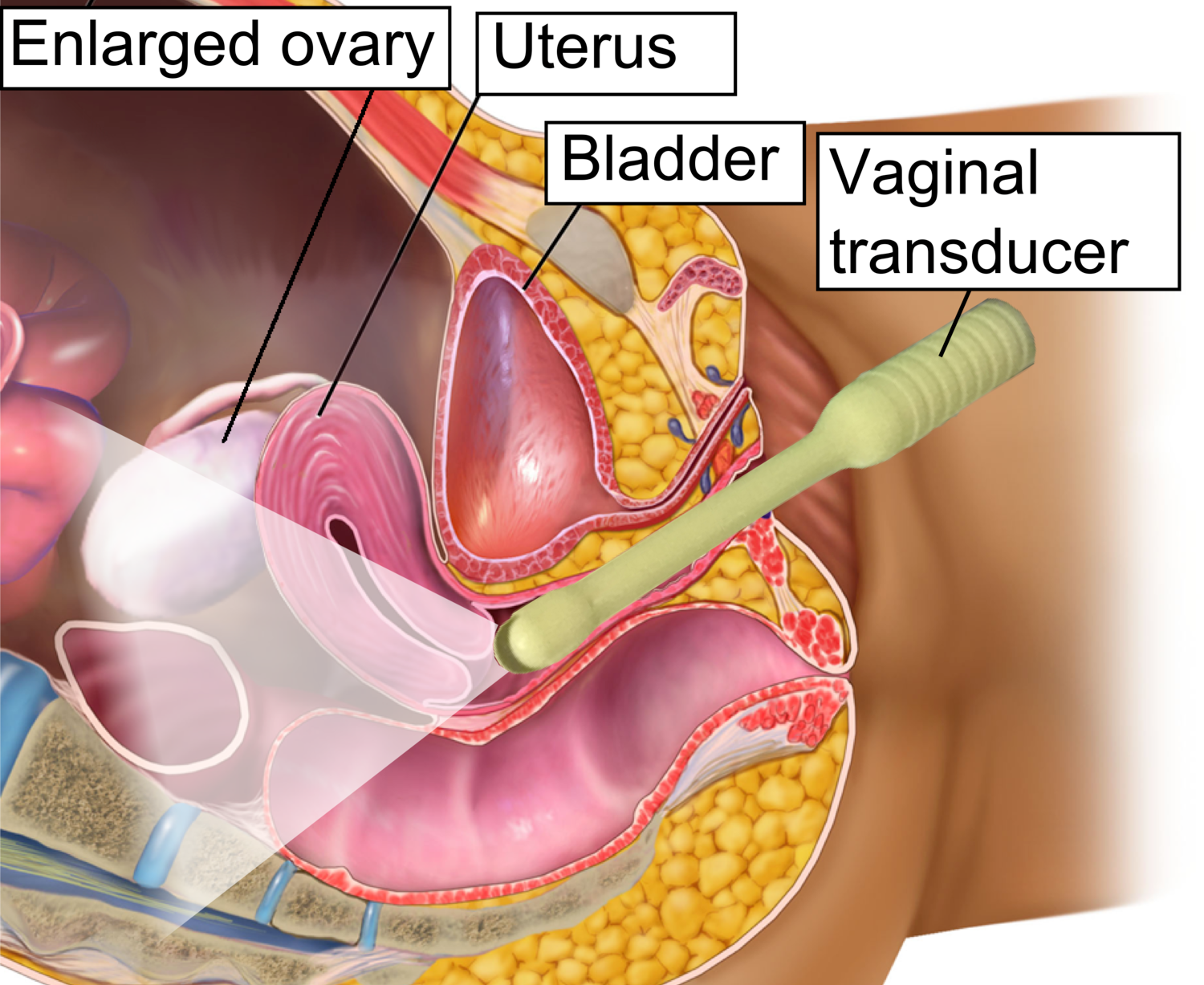
Dr. Michael Wynn-Williams offers specialized transvaginal ultrasound (TVUS) for the detection and assessment of ovarian endometriomas, also known as “chocolate cysts,” which occur in approximately 17-44% of patients with endometriosis. Using advanced ultrasound expertise, Dr. Wynn-Williams can identify the characteristic features of endometriomas, including their typical “ground-glass” echogenicity from old menstrual blood and tissue. These cysts, which can range from small lesions to large masses exceeding 10cm, are readily diagnosed through TVUS when they display their classic unilocular or multilocular appearance with fewer than five locules and homogeneous low-level internal echoes. Dr. Wynn-Williams also assesses for associated findings such as ovarian mobility using the “sliding sign” technique and evaluates for the presence of “kissing ovaries” where bilateral endometriomas are adherent in the pouch of Douglas, which indicates severe pelvic adhesions and more extensive endometriotic disease requiring comprehensive surgical planning.
-
Endometriosis tissue that grows in the bowel (rectum, sigmoid, and sometimes the caecum) will often cause symptoms such as painful bowel motions (dyschezia), rectal bleeding, constipation, diarrhoea, and long skinny bowel motions (ribbon stools). In practised hands, bowel lesions can be seen quite clearly using TVUS. The ultrasound allows Dr Wynn-Williams to work out the size and number of bowel lesions present and give you several options for how to manage your symptoms. If you have nodules in the bowel that are larger than 3cm or multiple areas of bowel endometriosis, you may be referred to a colorectal surgeon as part of your management plan. The majority of lesions will be smaller than 3cm and will be managed by Dr Wynn-Williams himself. If the extent of the endometriosis in the bowel or bladder is seen to be extensive, then you may be referred for an MRI scan. Endometriosis on the small intestine cannot be seen on TVUS.
-
A pelvic ultrasound may not pick up the superficial endometriosis that the majority of women with endometriosis have, and that is why a laparoscopy may still be required despite a negative ultrasound. Often, pelvic ultrasounds are performed by sonographers and or reported by radiologists who do not have experience in finding and locating superficial or deep infiltrating endometriosis. A negative transvaginal ultrasound does not rule out the presence of pelvic or extrapelvic endometriosis. If you have symptoms and are concerned about endometriosis, it is essential that someone with extensive experience in the field performs your pelvic ultrasound.
Dr Wynn-Williams will work with you to diagnose and treat your endometriosis and pelvic pain, using the latest in advanced ultrasound and surgical techniques.

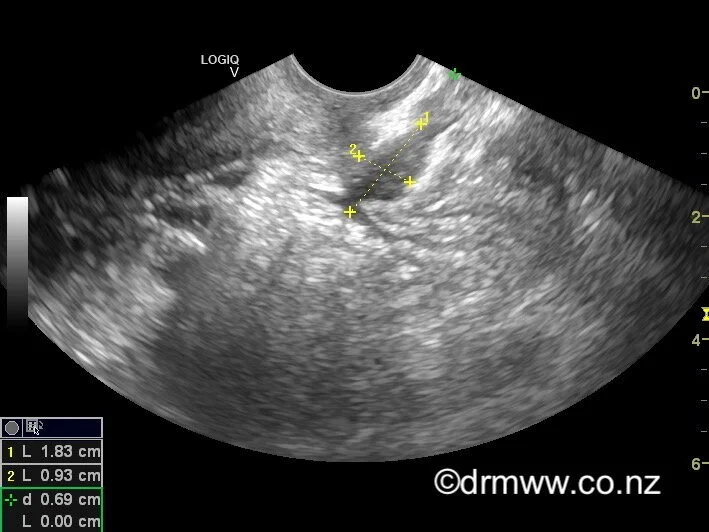
Rectal Muscularis Endometriosis nodule seen on TVUS
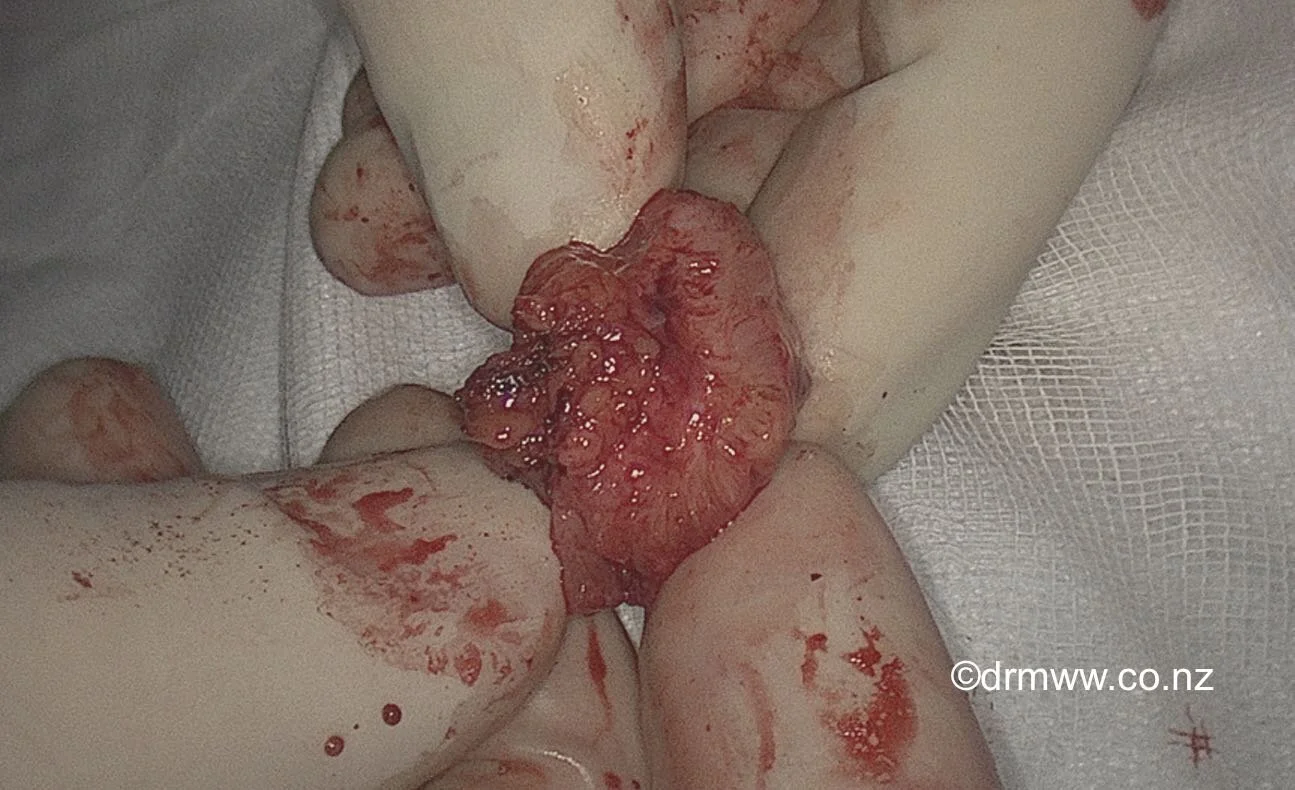
A rectal muscularis lesion after laparoscopic shaving
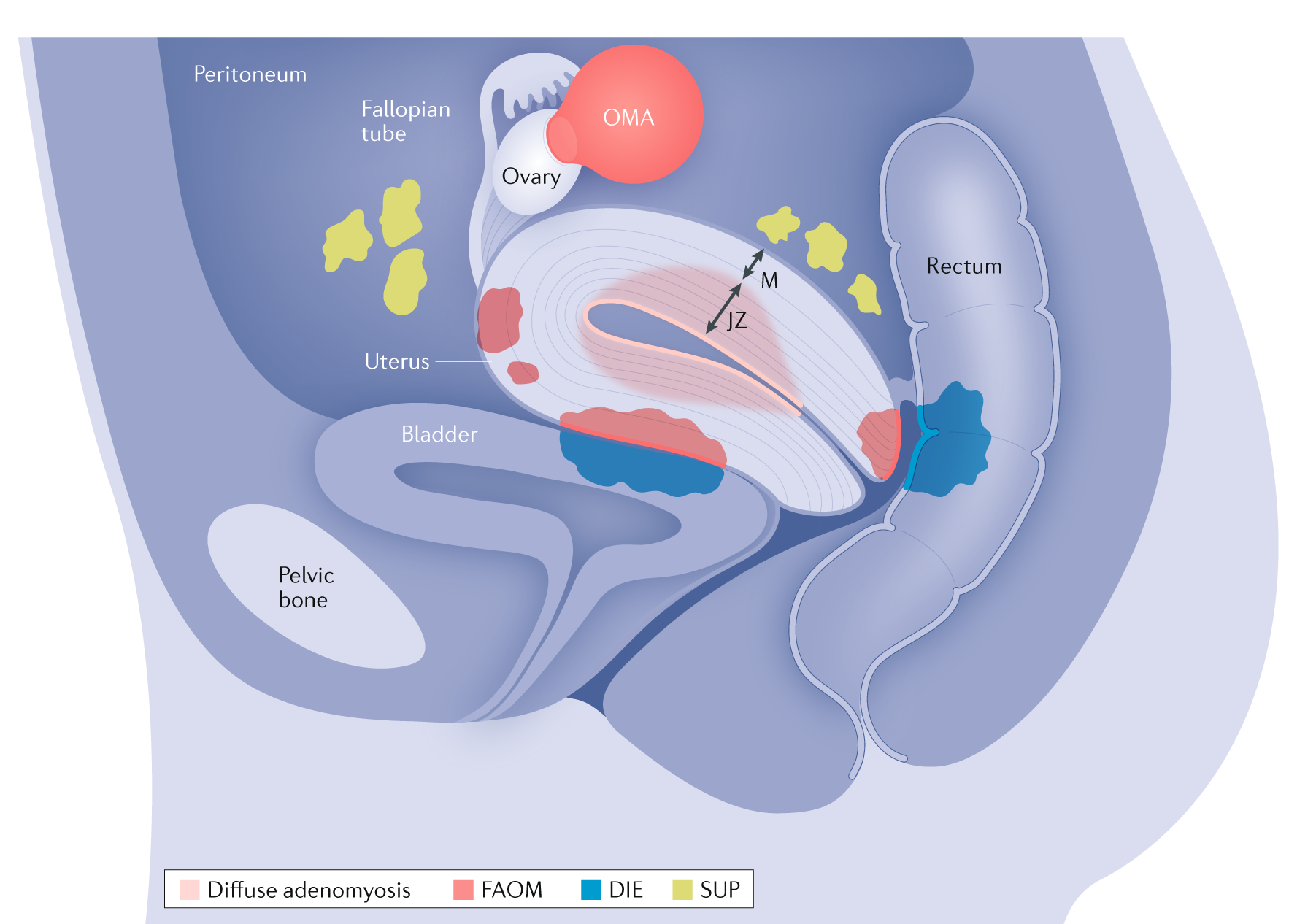
Areas on DIE that can be seen on TVUS

Dr Michael Wynn-Williams
MBChB (Otago), FRANZCOG
Gynaecologist, Advanced Laparoscopic Surgeon, Endometriosis and Pelvic Pain Specialist
Dr Michael Wynn-Williams is a highly experienced Auckland gynaecologist and laparoscopic surgeon, specialising in the treatment of endometriosis, fibroids, pelvic pain, and ovarian cysts. With a commitment to minimally invasive surgery and evidence-based practice, he helps women across New Zealand achieve better outcomes with empathy, precision, and respect